Chest Wall Resection and Reconstruction in a Dog with a Grade I Chondrosarcoma
Signalment: 14-year-old, MN mixed breed dog
History:
A firm mass was noted by the owner on the left ventrolateral chest wall and the mass had slowly grown over a 3-month period.
Physical exam findings:
58.9 mm x 42.7 mm firm and fixed mass on the left ventrolateral cranial thoracic wall
Diagnostic and clinical staging tests:
CBC: no abnormalities
Serum biochemistry: mildly increased ALP
Fine-needle aspirate: suspected sarcoma
CT scan: Soft tissue mass, 4.4 cm x 5.0 cm x 5.8 cm, centred around the proximal aspect of the costochondral junction of the left fourth rib with possible involvement of the fifth rib. No evidence of lung metastasis.
Notes:
The owners and I had a detailed discussion about the difference in prognosis between primary rib osteosarcoma (median survival time 120-190 days with surgery alone and 240-290 days with surgery and chemotherapy) and chondrosarcoma (median survival time 1080 to >3820 days with surgery alone), the two most common primary rib tumors in dogs. We also discussed the two main reasons to do a preoperative biopsy: 1. If the results change what me, as the clinician, recommends, or 2. If the results change the owners’ willingness to proceed with treatment. The results of a biopsy would not change my treatment recommendation as a chest wall resection and reconstruction would be recommended regardless of tumor type; however, with the marked differences in prognosis, the biopsy results may change the willingness of the owner to proceed with chest wall resection. In this case, the owners decided to proceed with surgery without doing a preoperative biopsy.
Treatment:
Chest wall resection with one normal rib cranially and caudally (third through sixth, four ribs in total) for cranial and caudal margins, 3 cm of normal rib dorsal to the tumor, and the costosternal junction (with an ipsilateral median sternotomy of the third through sixth sternebrae) for ventral margins. The chest wall defect was reconstructed with Marlex mesh, latissimus dorsi muscle flap, and pectoral muscle flap.
Outcome:
Grade I primary rib chondrosarcoma with complete histologic excision with ventral, dorsal, cranial, and caudal margins of 6.5 cm, 5.5 cm, 1.0 cm, and 1.4 cm, respectively.
No complications
Video link: https://www.youtube.com/watch?v=QQZOzGtYh7o (latissimus dorsi muscle flap only)
Tags: #ribCSA #chestwall #chestwallresection #chestwallresection #chondrosarcoma

Axial CT scan showing a left ventrolateral (costochondral junction) mass. The costochondral junction is a common location for primary rib tumors.

A multiplanar reconstruction of the CT scan shows that the rib mass is arising from the left fourth rib and there was partial involvement of the fifth rib. As a result, four rather than three ribs were planned to be resected.

A diagonal skin incision was made from cranioventral to caudodorsal, in the same direction as the latissimus dorsi muscle. This provides the best exposure of this muscle for dissecting it free and raising it for later reconstruction.

A Harmonic Scalpel was used to free the ventral border of the latissimus dorsi muscle.

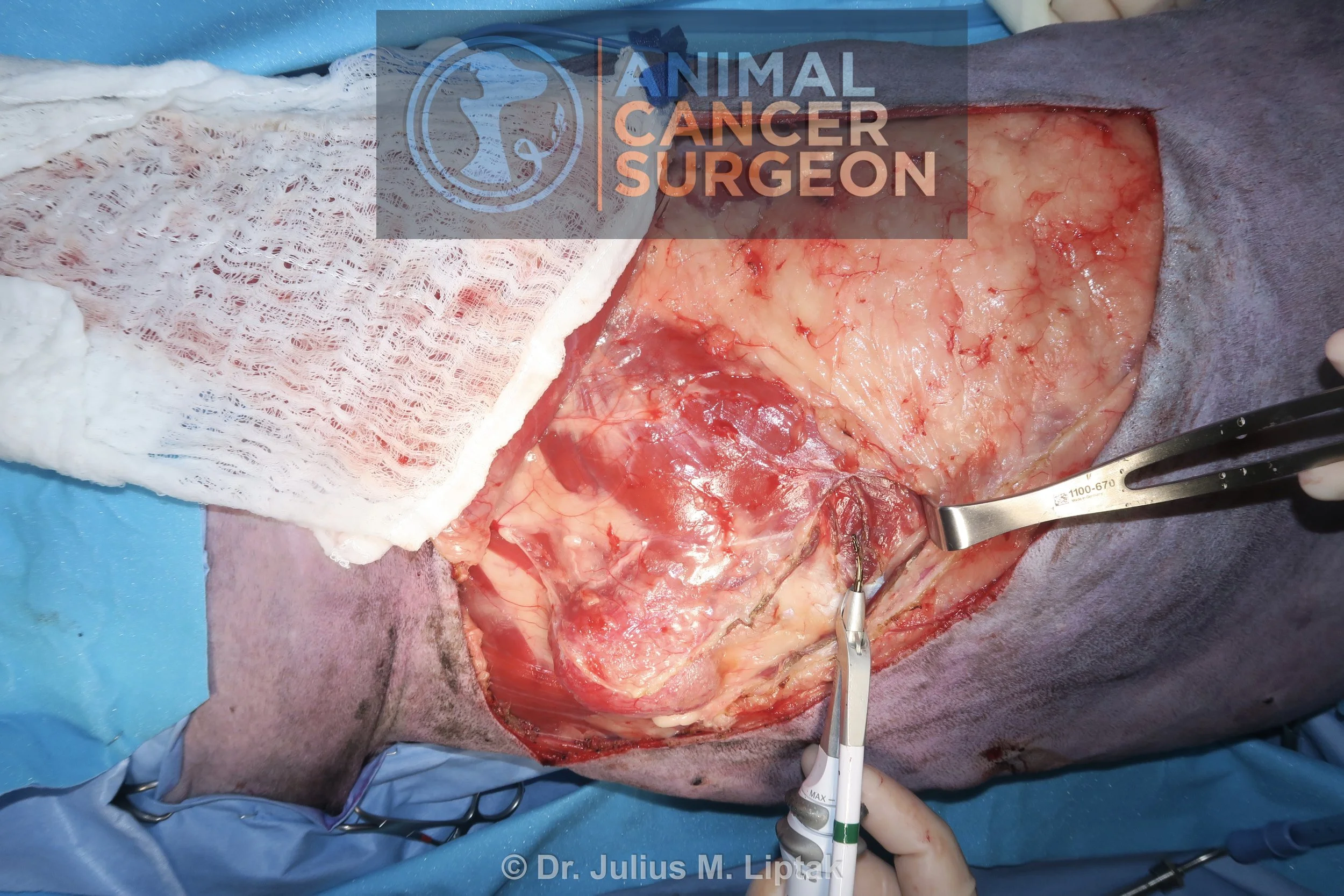
Once the ventral border of the latissimus dorsi was freed, it was elevated (pictured) and undermined. There are perforating vessels between the deeper chest wall and latissimus dorsi muscle which need to be sealed and transected.

Once the ventral border of the latissimus dorsi was freed, it was elevated and undermined (pictured). There are perforating vessels between the deeper chest wall and latissimus dorsi muscle which need to be sealed and transected.

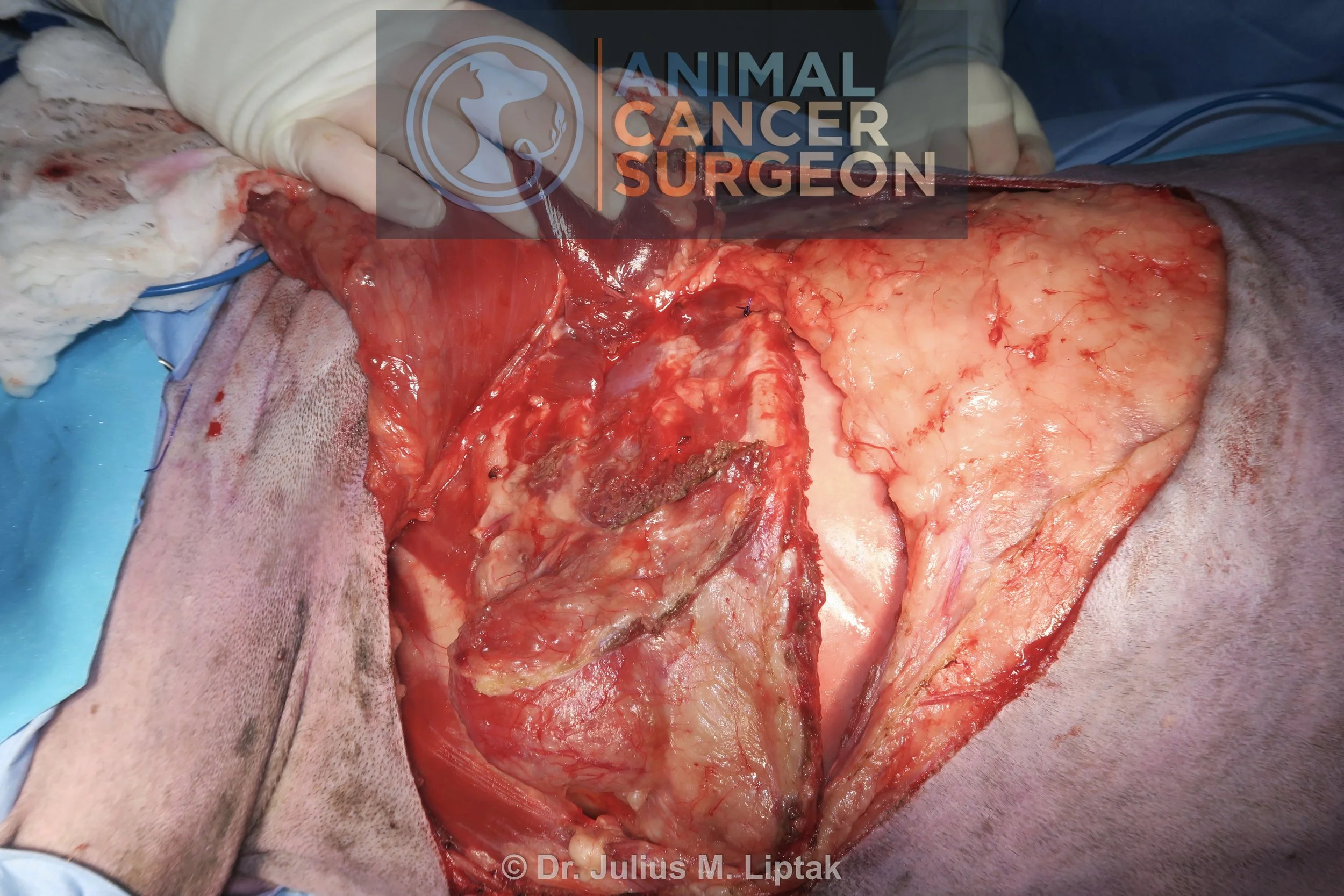
The latissimus dorsi muscle inserts on the 13th rib and this caudal border is then incised with a Harmonic Scalpel. Once this is elevated, the dorsal border (arrow) of the latissimus dorsi muscle is best visualized from the deep aspect of the muscle rather than superficially.

The dorsal border of the latissimus dorsi muscle was then incised and freed with a Harmonic Scalpel.

The latissimus dorsi muscle after the ventral, caudal, and dorsal borders were freed. Note the skin hooks used to atraumatically manipulate the muscle flap; these are made from hypodermic needles.
The first step for the chest wall resection, after raising the latissimus dorsi muscle, is performing an intercostal thoracotomy caudal to the first normal rib caudal to the rib tumor. In this case, the 6th-7th intercostal space.

Once the caudal intercostal thoracotomy is completed, the rib is retracted laterally to directly visualize the primary rib tumor, assess whether there is any obvious adhesion between the rib tumor and intrathoracic structures (such as the lung lobe or pericardium), and determine if any changes need to be made to the planned dorsal and ventral margins.

Once the caudal intercostal thoracotomy is completed, the rib is retracted laterally to directly visualize the primary rib tumor (arrow), assess whether there is any obvious adhesion between the rib tumor and intrathoracic structures (such as the lung lobe or pericardium; none in this case), and determine if any changes need to be made to the planned dorsal and ventral margins (none in this case).

Intraoperative image following completion of the caudal intercostal thoracotomy.

To prophylactically control bleeding from the intercostal vessels, a ligature (0 PDS) was passed circumcostally around the proximal aspect of the 6th rib.

To prophylactically control bleeding from the intercostal vessels, a ligature (0 PDS) was passed circumcostally around the proximal aspect of the 6th rib.
To prophylactically control bleeding from the intercostal vessels, a ligature (0 PDS) was passed circumcostally around the proximal aspect of the 6th rib.

Once the circumcostal ligature is completed, the rib is ostectomized distal to the circumcostal ligature with bone cutters.

It ended up that I did not have enough Weeties to ostectomize the ribs with bone cutters and subsequently had to resort to using a sagittal saw for the rib ostectomies.

The intercostal muscles between the 5th and 6th ribs were then transected with a Harmonic Scalpel.

The circumcostal ligature was secured and an ostectomy of the proximal aspect of the 5th rib was performed with a sagittal saw. This was repeated for the fourth and third ribs.

A second intercostal thoracotomy was performed cranial to the first normal rib cranial to the rib tumor (3rd rib), in this case a 2nd-3rd intercostal space.

The rib segment was reflected ventrally. The internal thoracic artery was sealed and transected with a Harmonic Scalpel. This allowed exposure of the ventral midline of the sternum. A median sternotomy was performed with a sagittal saw between the 3rd and 6th sternebrae, and the ipsilateral half of these sternebrae were resected en bloc with the chest wall segment. This was done because the rib mass was ventrally located and resecting the costochondral junction was deemed necessary to obtain adequate ventral margins, similar to what is done for resection of appendicular bone tumors.

The chest wall defect of four ribs following removal of the resected chest wall segment.

A double layer of Marlex was secured to the corners of the chest wall defect with tagging sutures (using 0 Prolene) to place the mesh under a degree of tension to provide rigidity to the chest wall reconstruction.

The mesh was then sutured to the edges of the chest wall defect using 0 Prolene in a simple continuous suture pattern.

The pectoral muscle was undermined, preserving its cranial and caudal insertions, to create a bipedicle flap. The bipedicle pectoral muscle flap was then pulled dorsally to cover the ventral aspect of the mesh.

The pectoral muscle was undermined, preserving its cranial and caudal insertions, to create a bipedicle flap. The bipedicle pectoral muscle flap was then pulled dorsally to cover the ventral aspect of the mesh.

The latissimus dorsi muscle was then transposed into the chest wall defect and sutured over the mesh to the cranial and caudal aspect of the defect and ventrally to the pectoral muscle flap.

Postoperative specimen image of the resected mass, a completely excised, grade I chondrosarcoma. The median survival time for dogs with primary rib chondrosarcoma varies from 1080 days to >3820 days. Unlike appendicular chondrosarcomas, histologic grade is not prognostic. The tumor-related mortality rate varies from 9% to 25%.

Postoperative specimen image of the resected mass, a completely excised, grade I chondrosarcoma. The median survival time for dogs with primary rib chondrosarcoma varies from 1080 days to >3820 days. Unlike appendicular chondrosarcomas, histologic grade is not prognostic. The tumor-related mortality rate varies from 9% to 25%.