liver tumors
BACKGROUND
Liver tumors are uncommon in cats and dogs. Liver tumors are defined by tumor type and gross morphology. Tumor types include hepatocellular carcinoma (HCC or hepatoma), bile duct adenoma (or cystadenoma) and adenocarcinoma, neuroendocrine carcinoma, various sarcomas (ie, hemangiosarcoma, histiocytic sarcoma, and leiomyosarcoma), and benign tumors such as myelolipoma. HCC is the most common liver tumor in dogs. Unlike people, HCC in dogs often have a benign biologic behaviour and some pathologists prefer to diagnose these as benign hepatomas. The benign bile duct cystadenoma is the most common liver tumor in cats. The liver is also a common site for metastasis from tumors in other locations. Gross morphology refers to the physical appearance of the tumor and is defined as massive (single large tumor), nodular (multiple tumors in more than one liver lobe), and diffuse.



DIAGNOSIS
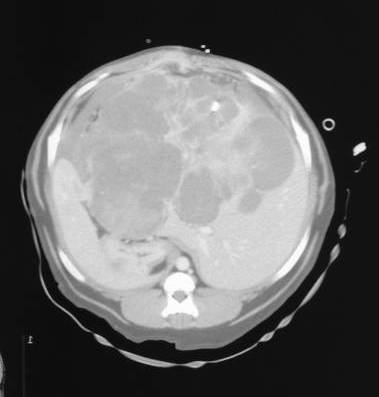
A contrast-enhanced CT scan of a massive HCC. This appeared unresectable on CT scan, but was resected following evaluation during an exploratory celiotomy.
Diagnostic tests include blood tests, abdominal ultrasound or CT scan, and aspirates or biopsies collected via ultrasound-guidance, laparoscopic, or open surgery. Triple-phase CT scans (precontrast phase, arterial phase, and portal venous phase) can be used to differentiate HCC from metastatic liver tumors from nodular hyperplasia; however, the ultrasonographic appearance of hepatic masses is highly variable and cannot be used to differentiate tumor types and malignant from benign disease. For tumors with massive morphology and no evidence of metastasis, surgical resection without preoperative biopsy is acceptable because knowledge of tumor type will not change treatment options.
Abdominal ultrasound or CT scan should not be used to determine resectability of massive liver tumors. Massive liver tumors are often large and can appear to unresectable when imaged with either ultrasound or CT scan. Direct examination and palpation during an exploratory celiotomy is the only way to definitively determine whether a liver mass is resectable or not.
CLINICAL STAGING
Thoracic radiographs or CT scans are recommended to assess for metastasis to the lungs. Abdominal ultrasound or CT scan is recommended for both diagnosis of a liver mass and also to evaluate for metastasis to other abdominal organs or lymph nodes.
TREATMENT
The only known effective treatment for liver tumors is surgical resection with liver lobectomy. This limits surgical resection to tumors with massive morphology and perhaps some nodular tumors. Right-sided liver tumors can be difficult to excise because of the proximity of the caudal vena cava.



There is no known effective treatment for cats and dogs with nodular and diffuse liver tumors as liver tumors are generally considered resistant to chemotherapy and radiation therapy. However, three-dimensional conformal radiation therapy has been reported with objective responses in five of six dogs and minimal acute radiation effects; and the use of adjuvant gemcitabine in dogs with incompletely excised massive HCC, nodular HCC, and diffuse HCC has been reported in 18 dogs with good results.
Palliative treatment options, especially for nodular and diffuse hepatic tumors, include, microwave ablation, embolization, and chemoembolization, but these modalities are not widely available.
PROGNOSIS
The prognosis following surgical resection of massive HCC in dogs and bile duct adenomas in cats is very good. The majority of cats and dogs are cured. In one study of 42 dogs with massive HCC treated with liver lobectomy, two dogs (5%) died intraoperatively secondary to blood loss as a result of iatrogenic trauma to the caudal vena cava; no dog developed local recurrence (despite four dogs having incomplete histologic excision of their tumor); two dogs (5%) developed suspected metastatic disease; and the remaining 38 dogs (90%) were either alive, lost to followup, or had died of unrelated reasons. The median survival time for dogs with massive HCC is > 1,460 days (ie, 90% of dogs were cured following surgery) and this was significantly better than the median survival time of 270 days for untreated dogs with untreated dogs 15.4-times more likely to die of tumor-related reasons. Poor prognostic factors include dogs not treated surgically with lung lobectomy, high preoperative ALT levels, high preoperative AST levels, high ALP-to-AST ratio, high ALT-to-AST ratio, and right-sided massive HCC. However, serum biochemical liver values and ratios have not been found to be prognostic in other studies, and right-sided liver tumors have a similar prognosis to central and left-sided liver tumors if dogs survive surgery.
The prognosis is guarded to poor for cats and dogs with malignant tumors other than HCC and any tumor with a nodular or diffuse morphology. In 18 dogs with incompletely excised massive HCC and incompletely excised or unresectable nodular HCC or diffuse HCC treated with adjuvant gemcitabine, the median survival times were 1339 days, 983 days, and 113 days, respectively. Nine of these dogs died of progressive disease and one of lung metastasis with the remaining dogs either lost to followup, alive, or dying of unrelated causes.
Massive Hepatocellular Carcinomas in Dogs and Cats




































Biliary Cystadenomas in Cats
















Biliary Carcinomas in Dogs and Cats






Primary Hepatic Sarcomas in Dogs






Last updated on 6th March 2017